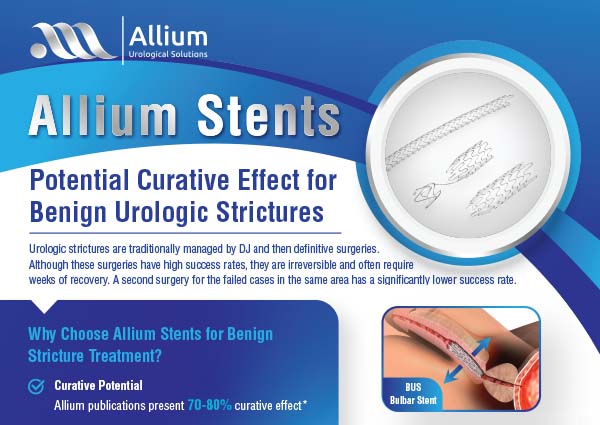
The Allium BUS stent is designed specifically for the treatment of recurrent strictures along the bulbar urethra. This new generation of bulbar stents is fully covered, self-expandable and large in caliber. Allium BUS matches the contours of the bulbar urethral lumen. The main body acts as a mold to allow forming a large urethral lumen, and the dynamic sphincteric segment preserves sphincteric functionality avoiding incontinence. The Allium BUS is intended for a long-term use of up to 3 years and is designed to be removed easily and safely even after this long indwelling period.
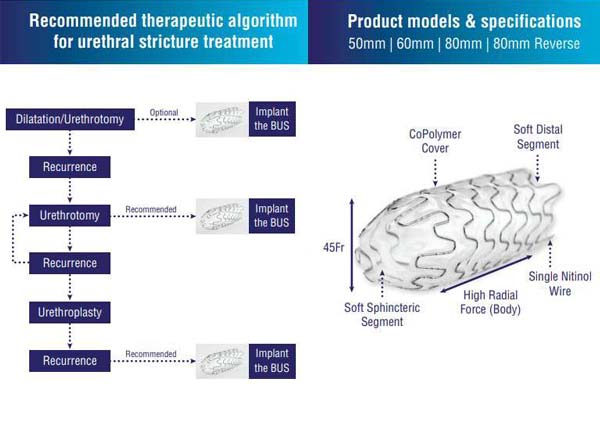
The Allium BUS stent can be used at any stage of treatment protocol for recurrent bulbar urethral stenosis:
- Replacing repeated dilations
- Replacing/avoiding repeated urethrotomies
- Prior to Bulbar urethroplasty
- Following failure of Bulbar urethroplasty
Studies have shown that after an optical urethrotomy, which acts as a dilation prior to stent implantation, Allium BUS can prevent recurrent stenosis in up to 80% of the patients with benign strictures. The optimal indwelling period to cure the bulbar urethral stenosis is 12 months. The BUS stent does not have any negative effect on the quality of the consecutive urethroplasty if needed. BUS is fully-retrievable, minimally invasive treatment of recurrent bulbar urethral obstruction.
Product Models
- Delivery system – the BUS is mounted on a rigid deployment system of 22Fr
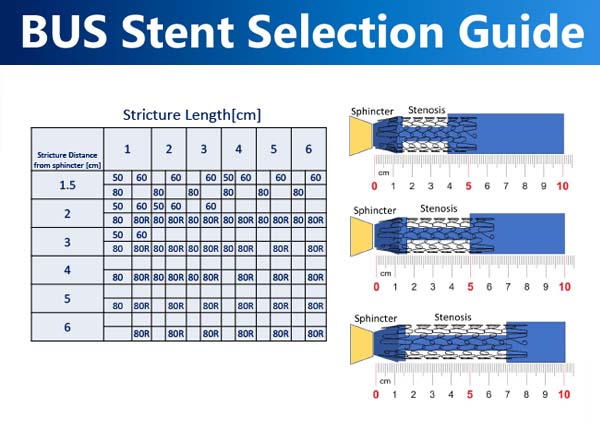
- Stent lengths available: 50mm, 60mm, 80mm and 80mm in reverse model (80-R) – all with 45 Fr caliber.


The Allium BUS stent's benefits
Long indwelling time of up to 3 years
Retrievable
Minimally invasive
Fully prevents tissue ingrowth
Easy insertion and stent positioning / repositioning
Superior patient comfort
Can be inserted either retrogradely or anterogradely
Easy removal of the device using alligator/rat tooth graspers
Unique anatomic design
Possible Curative effect of 70-80%
Click here for the brochure and relevant publications. Curative effect is not CE-Approved